The New Scramble for Africa: From the Berlin Conference to the "America First" Health Framework
Zimbabwe has formally rejected the "America First" Global Health Strategy, the $367 million aid package sounding like a modern reincarnation of the 1888 Rudd Concession.

Harare - In the deep-veined history of the African continent, the echoes of 1884 are growing louder. While the 19th-century "Scramble for Africa" was defined by steamships, Maxim guns and the ink of the Berlin Conference, the 21st-century iteration is being written in the clinical language of bilateral health Memorandums of Understanding (MoUs) and "America First" diplomatic frameworks.
The recent collapse of negotiations between the United States and Zimbabwe over the America First Global Health Strategy (AFGHS) goes beyond budgetary disputes, tracing a modern-day reenactment of the struggle for resource sovereignty that dates back to the Rudd Concession.
In 1884, fourteen nations gathered in Berlin to establish the "Principle of Effective Occupation," a protocol that legalized the partition of Africa without a single African present.
Today’s AFGHS, championed by the Donald Trump administration, utilizes a different but equally potent protocol known as Conditional Bilateralism.
While the strategy publicly promotes self-reliance and mutual accountability, the underlying contents reveal a transactional shift that observers have termed "extractive diplomacy."
Internal reports and analysis by Health Policy Watch, reveals that the AFGHS demands significant concessions in exchange for the continuation of critical life-saving aid.
A primary pillar of this strategy is Pathogen Sovereignty, where signatory nations must agree to a specimen sharing agreement, requiring them to surrender biological samples and genetic sequence data of pathogens to the U.S. within five days of detection.
Critics argue that this allows Western pharmaceutical giants to patent treatments derived from African pathogens without sharing the benefits.
Furthermore, the strategy mandates Digital Intelligence Access, which requires the integration of national health data into U.S.-driven digital architectures.
This grants Washington direct oversight of demographic and epidemiological data, a move security advisors in Harare labeled as intelligence overreach.
Most contentiously, the strategy increasingly links health funding to critical mineral frameworks. In countries like the DRC and Zambia, health aid has been discussed alongside preferential access to cobalt and lithium, minerals essential for U.S. national security and the global energy transition.
The Ghost of Lobengula: Zimbabwe’s Defiant No
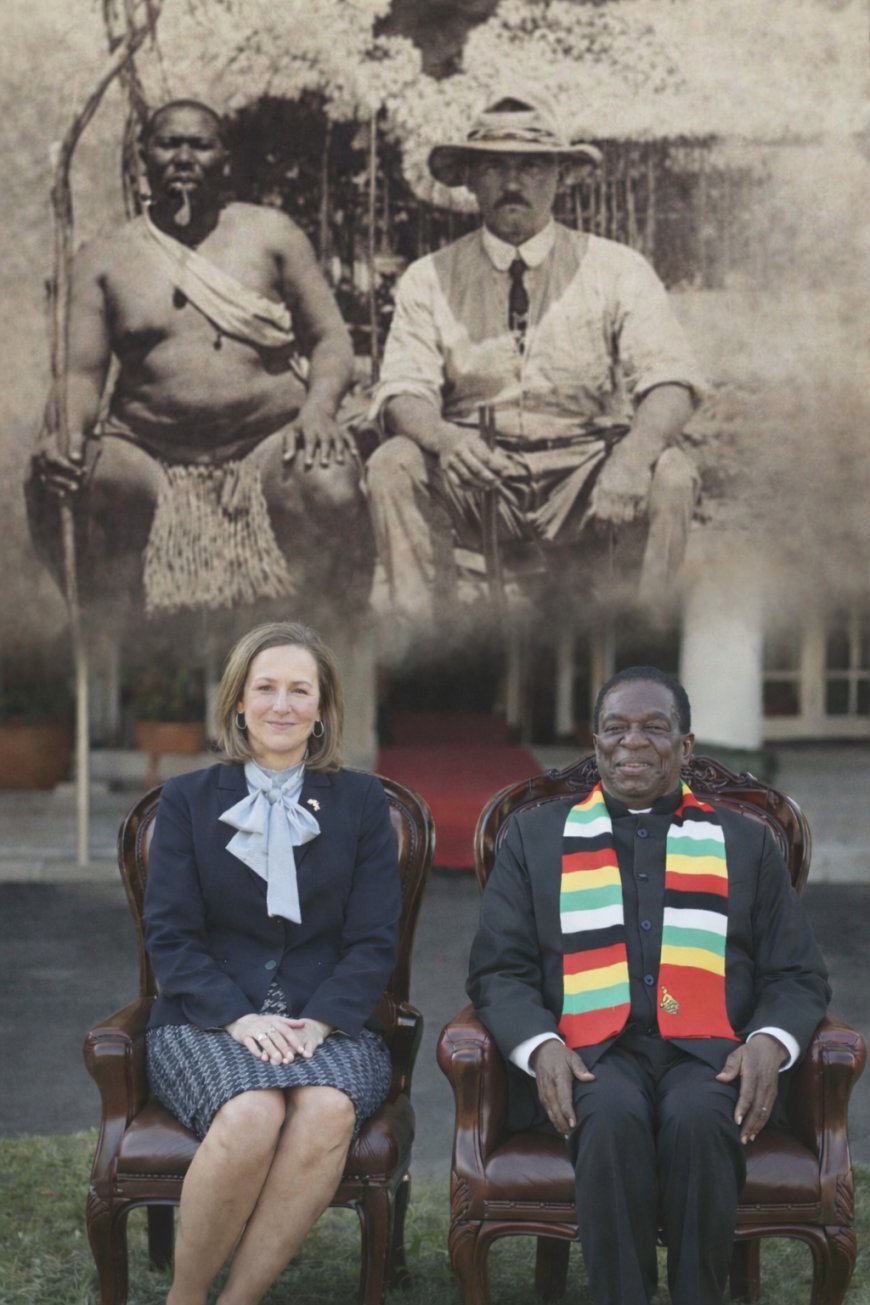
Nowhere is the historical parallel more striking than in Zimbabwe. In 1888, King Lobengula of the Ndebele signed the Rudd Concession, a document that granted Cecil John Rhodes’ agents exclusive power over all metals and minerals in his kingdom.
Lobengula was promised rifles, ammunition and a monthly stipend, believing he was granting a limited mining right. Instead, he had unknowingly signed away the sovereignty of what would become Rhodesia.
In 2026, President Emmerson Mnangagwa found himself facing a modern Rudd Concession. The U.S. offered a US$367 million health framework to sustain 1.2 million people on HIV treatment and other diseases.

The America First fine print however required Zimbabwe to grant strategic vantage points regarding its lithium and platinum reserves, bypass the World Health Organization’s multilateral data-sharing systems, and allow U.S. audits of national health facilities and laboratories.
Unlike Lobengula, who realized the deception too late, the Zimbabwean executive terminated the negotiations before the ink was dry.
Ambassador Albert Chimbindi, Secretary for Foreign Affairs, framed the refusal as a stand against a lopsided deal that blatantly undermines the sovereignty of Zimbabwe.
The government’s spokesperson, Nick Mangwana, argued in The Herald that the deal was a trap, noting that the nation would provide the raw materials for scientific discovery without any assurance that the end products would be accessible to the Zimbabwean people.
The America First strategy creates a vivid fairness gap that mirrors the colonial protocols of the past. Under the AFGHS, African nations are required to progressively cover nearly all frontline health costs, including commodities and staff, while the U.S. retains control over the intellectual property and data.
This shift from the 1888 era, where bilateral concessions traded total mineral rights for rifles and stipends, to the 2026 era, where health MoUs trade pathogen data and mineral access for medical supplies, highlights a consistent theme of asymmetrical exchange, durables for perishables.
Across the continent, the response is fractured. While some nations have signed variations of these agreements to avoid a sudden funding cliff, others have refused just like Zimbabwe.
The Africa Centre for Disease Contro (CDC) has recently pushed for Health Sovereignty, urging member states to prioritize the WHO’s multilateral Pathogen Access and Benefit-Sharing (PABS) system over bilateral deals, like the U.S., to ensure that the benefits of scientific research are shared equitably.
The U.S. wind-down of aid in Zimbabwe marks a definitive end to the era of purely humanitarian assistance. By treating health aid as a commodity to be traded for minerals and data, the America First strategy has stripped the mask of altruism from global diplomacy.
The Zimbabwe decision to reject the deal is a high-stakes gamble that leaves a US$367 million hole in the health budget and puts 1.2 million lives at risk.
The Architecture of Intermediaries: Rhodes’ Agents vs. Modern "Implementers"
A pivotal similarity lies in the removal of direct state-to-state accountability. In 1888, Cecil Rhodes did not negotiate with King Lobengula himself; he sent Charles Rudd, Rochfort Maguire and Francis Thompson, private agents of a commercial interest that would later become the British South Africa Company (BSAC). This allowed the British Crown to benefit from the extraction while maintaining "plausible deniability" regarding the deceptive tactics used to secure the signature.
Under the AFGHS, a parallel structure has emerged. Washington’s strategy increasingly bypasses central government Ministries in favor of private "implementing partners" and U.S.-based NGOs. Though some sections of the Zimbabwe civil society argue that this is for transparency and accountability purposes to protect civil funding from diversion by government, funneling the US$367 million through third-party contractors rather than national systems, the U.S. effectively creates a "shadow health state."
Like the BSAC agents of the 19th century, these modern implementers serve as the frontline for data extraction, harvesting Zimbabwean pathogen samples and demographic insights for private pharmaceutical databases under the guise of technical assistance.
The Rudd Concession was secured by the promise of 1,000 Martini-Henry rifles, a technology that gave the Ndebele a temporary sense of security but was ultimately used to ensure their subjugation. In the 2026 AFGHS framework, the "rifles" are replaced by proprietary medical technologies and vaccines.

The "fine print" of the AFGHS however creates a closed loop of intellectual property, manifesting scientific imperialism or research colonialism. By demanding real-time access to Zimbabwe’s unique viral and bacterial genetic sequences, the U.S. positions its private sector to patent treatments derived from African biology, with some sections of Africa fearing development of ethnic bioweapons, gene customised targetted biological weapons.
This mirrors the 1888 arrangement, where Zimbabwe provides the "raw material" (biological data/minerals), while the foreign power retains the "technology" (patents/rifles).
The result is a cycle where the host nation must eventually buy back the cure for its own diseases at a premium, just as Lobengula’s rifles required the constant purchase of British-made ammunition to remain functional.
The Protocol of Encirclement: Economic Isolation as a Tool
Historians note that Lobengula was pressured into the Rudd Concession through strategic encirclement, Rhodes ensured that other competing powers, the Portuguese and Boers, were blocked or bribed, leaving the King with no other choice but the British deal.
The AFGHS employs a digital and fiscal version of this encirclement. By withdrawing from the World Health Organization (WHO) and attacking multilateral funding mechanisms, the "America First" strategy seeks to eliminate the "other choices" available to African nations.
The recent withdrawal of aid from Zimbabwe is a tactical message to the rest of the continent that those who do not accept the bilateral "co-investment" model and the mineral concessions attached to it, will be left in a state of clinical isolation.
The diplomatic siege is designed to break the collective bargaining power of the Africa CDC and force individual nations back into the lopsided bilateralism of the 19th century, which 16 countries have already signed.